Chronic liver diseases (CLDs) affect nearly two billion people worldwide, making them a major global health burden. While much attention has been directed at cirrhosis, hepatitis, and non-alcoholic fatty liver disease (NAFLD), a less discussed but clinically significant complication is erectile dysfunction (ED). The intersection of these two conditions is not accidental: liver pathology profoundly disturbs hormonal metabolism, vascular function, and psychological well-being—all essential for sexual health. This article examines the epidemiology, mechanisms, and treatment approaches for ED in men with CLDs, drawing from recent research and highlighting the potential role of therapies such as sildenafil.
The Overlooked Burden of Erectile Dysfunction in Liver Disease
Erectile dysfunction is one of the most common male sexual disorders, affecting up to half of men aged 40–80 globally. In the context of chronic liver disease, its prevalence is significantly higher, ranging from 24% to 85% depending on etiology and disease stage. Men with cirrhosis, viral hepatitis, or NAFLD are particularly vulnerable, often experiencing progressive worsening of erectile capacity as liver function declines.
What makes this association particularly striking is its bidirectionality. ED is not merely a byproduct of liver disease; it may serve as an early marker of systemic dysfunction. For example, endothelial impairment, a hallmark of portal hypertension, compromises penile vascular response in much the same way it drives ascites and variceal bleeding. Likewise, metabolic syndrome—commonly present in NAFLD—creates a vicious cycle of insulin resistance, obesity, and vascular damage that exacerbates both liver disease and ED.
Despite these overlaps, erectile dysfunction remains underdiagnosed in hepatology clinics. Patients are often too focused on “serious” complications such as ascites or encephalopathy to mention sexual issues. Physicians, too, may neglect the topic. Yet ignoring ED overlooks an important dimension of quality of life—and potentially an early clinical signal of systemic decline.
Epidemiology Across Liver Disease Subtypes
The relationship between erectile dysfunction and chronic liver disease varies depending on etiology.
- Non-Alcoholic Fatty Liver Disease (NAFLD): With a global prevalence of ~25%, NAFLD is now the most common chronic liver disorder. Up to two-thirds of NAFLD patients report ED, a prevalence nearly three times higher than the general population. This association is largely driven by shared risk factors: obesity, diabetes, and hypertension.
- Cirrhosis: In cirrhotic patients, ED prevalence approaches 80%, especially in advanced or decompensated stages. Portal hypertension itself has been identified as an independent predictor of ED, underscoring the hemodynamic roots of dysfunction.
- Chronic Viral Hepatitis (HBV, HCV): Prevalence ranges from 14% to 78%. HCV appears to be more strongly linked with ED than HBV, possibly due to its inflammatory effects on vascular endothelium and associations with cryoglobulinemia.
- Alcoholic Liver Disease: The data are mixed. Some studies attribute ED directly to ethanol toxicity on the gonads, while others suggest cirrhosis rather than alcohol per se drives dysfunction.
Such variability underscores that ED is not a uniform complication of CLDs but rather a syndrome shaped by overlapping risk factors, disease stage, and comorbidities.
Mechanisms: Why Liver Disease Leads to Erectile Dysfunction
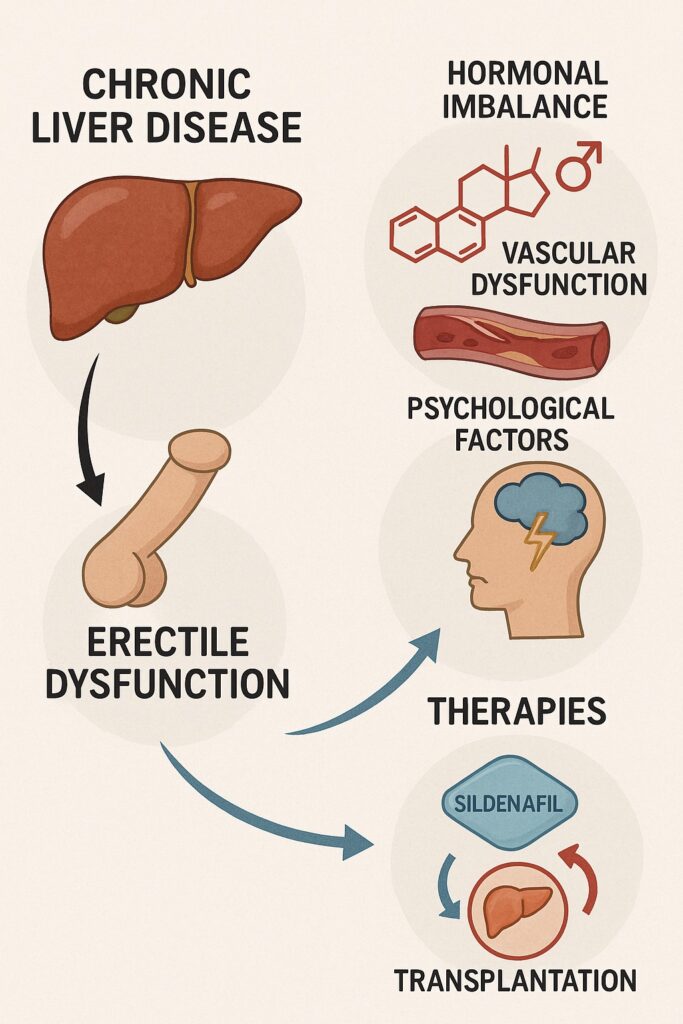
The liver is not traditionally thought of as a sexual organ, but its centrality in metabolism makes it a silent orchestrator of sexual health. Multiple pathways connect CLDs to ED:
Hormonal Disruption
The liver metabolizes sex hormones. In cirrhosis and NAFLD, impaired hepatic clearance leads to elevated estrogen and reduced testosterone. Hypogonadism, testicular atrophy, and feminizing features such as gynecomastia are common. Testosterone decline impairs nitric oxide synthase activity and increases cavernosal smooth muscle apoptosis, undermining erection.
Vascular and Hemodynamic Changes
Portal hypertension and systemic hyperdynamic circulation alter splanchnic blood flow, impairing penile perfusion. Endothelial dysfunction reduces nitric oxide bioavailability, preventing smooth muscle relaxation. Anemia, common in advanced CLDs, compounds the problem by reducing oxygen delivery to penile tissues.
Inflammation and Oxidative Stress
Chronic viral hepatitis and NAFLD generate systemic inflammation, with elevated cytokines (TNF-α, IL-6) suppressing gonadal function and accelerating endothelial damage. Oxidative stress contributes further by damaging cavernosal smooth muscle and endothelial cells.
Medications
Several treatments for CLDs worsen ED. Non-selective beta-blockers used for portal hypertension, SSRIs for depression, spironolactone, and interferon therapy all carry risk of sexual dysfunction.
Mental Health
Depression and anxiety are common in patients with CLDs and exert independent negative effects on sexual desire and performance. This psychosocial burden creates a feedback loop that worsens ED and reduces quality of life.
Clinical Implications and Therapeutic Opportunities
Treating erectile dysfunction in men with CLDs is complex but essential. The therapeutic landscape includes both direct interventions for ED and indirect strategies addressing underlying liver dysfunction.
PDE5 Inhibitors
Phosphodiesterase type 5 inhibitors (e.g., sildenafil, tadalafil) remain the mainstay of pharmacologic therapy. They enhance cGMP-mediated smooth muscle relaxation, restoring erectile capacity. Evidence suggests that PDE5 inhibitors can be safely used in patients with compensated cirrhosis (Child-Pugh A and B), though caution is advised in severe impairment. Small clinical trials report significant improvements in IIEF scores among cirrhotic patients treated with tadalafil or sildenafil, without major adverse hepatic effects.
Liver Transplantation
For eligible patients, transplantation not only restores hepatic function but also improves sex hormone metabolism and erectile capacity. Studies report significant increases in testosterone and IIEF-5 scores post-transplantation.
Adjunctive Strategies
- L-arginine supplementation may improve NO synthesis.
- Branched-chain amino acids support protein metabolism and have been linked to improvements in erectile function.
- Psychological support and therapy are critical for addressing depression, anxiety, and relationship strain.
Multidisciplinary care is key. Hepatologists, urologists, and mental health professionals must work together to optimize both liver health and sexual well-being.
Looking Ahead: Research Gaps and Future Directions
Despite clear associations, research into ED among CLD patients remains limited. Most studies are small, cross-sectional, and confounded by comorbidities. Future work must include:
- Large-scale randomized controlled trials testing PDE5 inhibitors specifically in CLD populations.
- Studies evaluating how improving liver disease (through transplantation, antifibrotic therapies, or lifestyle modification) impacts ED.
- Mechanistic research into pathways linking inflammation, oxidative stress, and hypogonadism in liver-related ED.
Until then, clinicians must rely on judicious use of existing tools, keeping sildenafil and related therapies in their arsenal while cautiously navigating hepatic safety.
FAQ
1. How common is erectile dysfunction in men with chronic liver disease?
Depending on the type and severity of liver disease, between one-quarter and four-fifths of men with CLDs experience ED. Cirrhosis and NAFLD show the highest prevalence.
2. Can sildenafil be used safely in patients with liver disease?
Yes, in most cases of mild to moderate liver impairment. Clinical studies show sildenafil and tadalafil can improve erectile function in cirrhotic patients without worsening portal hypertension, though dosing caution is advised in advanced disease.
3. Does liver transplantation cure erectile dysfunction?
Not universally, but transplantation significantly improves hormone balance and erectile capacity in many men, making it the most effective “curative” approach.
4. Are psychological factors also important in CLD-related ED?
Absolutely. Depression and anxiety are common in CLD patients and independently worsen ED. Addressing mental health is as important as treating hormonal or vascular factors.
📌 Chronic liver disease and erectile dysfunction share more than an incidental relationship. Their convergence reflects the systemic nature of liver pathology. By addressing both conditions in tandem—using therapies like sildenafil alongside holistic liver care—clinicians can restore not only health but dignity and intimacy to affected men.